ADIPS Poster Presentation Australasian Diabetes in Pregnancy Society and Society of Obstetric Medicine Australia and New Zealand Joint Scientific Meeting 2025
An Analysis of the Effectiveness of Initial Insulin Dosage for Gestational Diabetes (#126)
Background
There are no guidelines for determining initial insulin doses for women with gestational diabetes (GDM). We recently adopted Health2Sync, a web-based platform capturing blood glucose levels (BGs) from patient glucometers, and records insulin prescribed. We sought to determine the effectiveness of different insulin starting doses in improving BG.
Methods
Data from women with GDM at Westmead Hospital from July 2024-June 2025 were extracted from Health2Sync. Treatment targets were fasting BG <5.5mmol/L, and 2 hours postprandial <7.0mmol/L. BGs one week prior to and one week post-commencing rapid-acting analogue insulin (Lispro or Aspart) for breakfast, lunch and dinner, and/or bedtime NPH or Glargine, were compared. The main outcome was the percent of BGs above target in the week before and after commencing insulin.
Results
There were 263 women with GDM and insulin data. Those with incomplete data were excluded. The table shows the percent of BGs above target before and after commencing different insulin doses.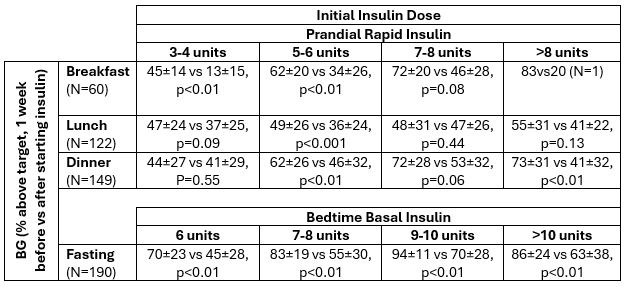
One patient had BG <4mmol/L after starting breakfast insulin (lowest 3.9mmol/L with 4 units), three after lunchtime insulin (lowest 3.2mmol/L with 6 units) and none after dinnertime or bedtime insulin.
Further analyses indicated that starting insulin doses and their effectiveness were influenced by mean pre-insulin BG levels but generally not by BMI.
Conclusion
Based on our data, for breakfast, 3-4 units is a reasonable rapid-acting insulin starting dose, whereas for dinner, 5-6 units is needed. With bedtime basal insulin, 6 units is effective, but given the lack of hypoglycaemia, larger starting doses are reasonable.