SOMANZ Poster Presentation Australasian Diabetes in Pregnancy Society and Society of Obstetric Medicine Australia and New Zealand Joint Scientific Meeting 2025
Medulloblastoma in pregnancy (#169)
Case
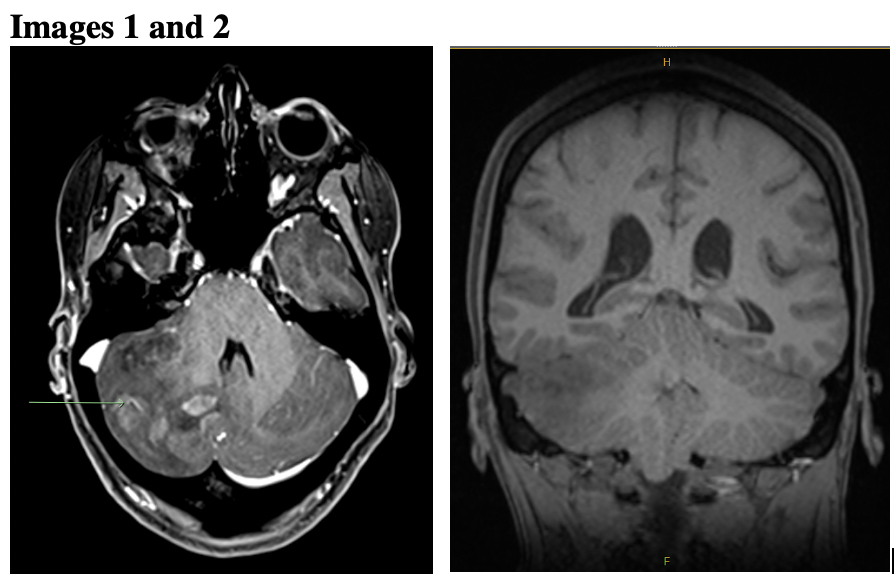
A 34-year-old primigravida woman presented at nineteen weeks’ gestation with progressive headaches and nausea. Cranial MRI revealed a 65x58x29mm right cerebellar mass with obstructive hydrocephalus and tonsillar protrusion below foramen magnum (Images 1 and 2). Initial treatment was dexamethasone and two stereotactic resections of cerebellar tumour, with significant residual cranial disease postoperatively. Histopathology revealed WHO CNS Grade 4 medulloblastoma with leptomeningeal metastases. Multidisciplinary consultation was undertaken with the woman, radiation and medical oncologists, neonatologists, neurosurgeons and obstetricians. She elected to continue the pregnancy. Proton pencil beam scanning craniospinal irradiation was not available. Cranial radiotherapy proceeded from 27 weeks’ gestation, and elective caesarean performed at twenty-nine weeks’ gestation to facilitate autologous stem cell harvesting and cranio-spinal radiotherapy. Adjuvant chemotherapy is planned to commence after completion of six weeks of radiotherapy.
Discussion
Medulloblastoma occurs predominantly in children, accounting for an estimated 1% of primary CNS tumours in adults. Fewer than 20 cases are described in pregnancy, with no specific management guidelines.1,2 Treatment during pregnancy consisted of partial or total resection in 10 women, and radiotherapy in one woman. None received chemotherapy during pregnancy. One pregnancy was associated with placental without foetal metastasis. The safety of chemotherapy and radiotherapy during pregnancy, and the importance of a multidisciplinary team approach in enabling the mother to make informed decisions regarding management will be discussed.3,4
- Paslaru FG, Panaitescu AM, Nestian E, et al. Medulloblastoma Presenting as Severe Headache during Pregnancy: A Case Report and Review of the Literature. Medicina. 2022;58(1):127. doi:https://doi.org/10.3390/medicina58010127
- Sendy F, Arrighi M, Berton Q, et al. Diagnosis of medulloblastoma in pregnant women: To continue with the pregnancy or not? A case report and literature review. Neurochirurgie. 2023;69(3):101443. doi:https://doi.org/10.1016/j.neuchi.2023.101443
- Cardonick E, Gringlas M, Hunter K, Greenspan JS. Development of children born to mothers with cancer during pregnancy: comparing in utero chemotherapy-exposed children with nonexposed controls. American Journal of Obstetrics and Gynecology. 2015;212(5):658.e1-658.e8. doi:https://doi.org/10.1016/j.ajog.2014.11.032
- Eastwood‐Wilshere N, Turner J, Oliveira N, Morton A. Cancer in Pregnancy. Asia-Pacific Journal of Clinical Oncology. 2019;15(6):296-308. doi:https://doi.org/10.1111/ajco.13235